Nosokinetics
Issue 41 February 2007
(c)Authors for content; Peter Millard, Roy Johnston for e-version
(comments to rjtechne at iol dot ie)We have a paper in full as well as the following reviews.
Adelaide 2006 Reviews
Seven papers from Adelaide 2006 in the February Issue of Australian Health Review:O’Doherty, K. C. (2007). Implications of conflicting definitions of probability to health risk communication: a case study of familial cancer and genetic counselling. Australian Health Review 31(1): 24-33.
The question of what probability actually is has long been debated in philosophy and statistics. Although the concept of probability is fundamental to many applications in the health sciences, these debates are generally not well known to health professionals. This paper begins with an outline of some of the different interpretations of probability. Examples are provided of how each interpretation manifests in clinical practice. The discipline of genetic counselling (familial cancer) is used to ground the discussion.
In the second part of the paper, some of the implications that different interpretations of probability may have in practice are examined. The main purpose of the paper is to draw attention to the fact that there is much contention as to the nature of the concept of probability. In practice, this creates the potential for ambiguity and confusion. This paper constitutes a call for deeper engagement with the ways in which probability and risk are understood in health research and practice.
Aust Health Rev 2007: 31(1): 24-33
Kumar, S. and K. Grimmer-Somers (2007). A synthesis of the secondary literature on effectiveness of hospital avoidance and discharge programs. Australian Health Review 31(1): 34-49.
The objective of this systematic review of the literature was to synthesise secondary evidence for hospital avoidance and discharge programs, compared with usual hospital care. Seventeen electronic databases were searched to identify relevant secondary peer-reviewed and grey research. Forty-eight publications were included.
Generally, evidence for safety, effectiveness and efficiency of hospital avoidance and discharge programs was equivocal, while there was encouraging evidence regarding improved patient-centred outcomes with most hospital avoidance and discharge planning interventions.
Aust Health Rev 2007: 31(1): 34-49
Rae, B., W. Busby, et al. (2007). Fast-tracking acute hospital care - from bed crisis to bed crisis. Australian Health Review 31(1): 50-62.
We describe here the results of a continuous quality improvement (CQI) project, the Delayed Discharge Project, in a general medicine service in a New Zealand teaching hospital. Average length of stay (ALOS) dropped by 2.6 days (6.5 to 3.9), readmission rates did not rise, costs of service delivery dropped by $2.4 million, patient numbers increased by 145 (2445 to 2590), while bed numbers reduced from 56 to 32 and ward outliers all but disappeared, suggesting success.
However, 2 years after the successful cost-saving measures were introduced the new system crashed as a result of additional bed closures and organisational restructures.
Aust Health Rev 2007: 31(1): 50-62
Campbell, J. A. (2007). Designing a podiatry service to meet the needs of the population: a service simulation. Australian Health Review 31(1): 63-72.
A model of a podiatry service has been developed which takes into consideration the effect of changing access criteria, skill mix and staffing levels (among others) given fixed local staffing budgets and the foot-health characteristics of the local community. A spreadsheet-based deterministic model was chosen to allow maximum transparency of programming. This work models a podiatry service in England, but could be adapted for other settings and, with some modification, for other community-based services.
The model enables individual services to see the effect on outcome parameters such as number of patients treated, number discharged and size of waiting lists of various service configurations, given their individual local data profile. The process of designing the model has also had spin-off benefits for the participants in making explicit many of the implicit rules used in managing their services.
Aust Health Rev 2007: 31(1): 63-72.
Bain, C. A. and L. K. Au (2007). A framework to provide clarity in the use of predictive technologies in health care management. Australian Health Review 31(1): 73-82.
This paper reports on a survey of health care managers and other stakeholders which assesses the need for a framework regarding predictive technologies in health care management. In the context of this paper, predictive technologies are defined as those that enable an insight into, or measurement of, events yet to occur. A framework could include the ability to classify the problems confronting managers, and the range of possible tools and techniques that could be used to address those problems. This could be of mutual benefit to health care managers, technologists and modellers.
The survey was intended to clarify the level of interest in such a framework, and also the possible dimensions that it ought to contain. Our results indicate that there is strong support for a proposed framework, with 97% of respondents indicating that a framework would be possibly or very useful. The results also show a low level of background knowledge in relation to existing tools, techniques and technologies. The draft framework is also presented. It includes dimensions relating to problem and tool definitions, scenarios to be investigated and the findings of those investigations.
Aust Health Rev 2007: 31(1): 73-82.
Champion, R., L. D. Kinsman, et al. (2007). Forecasting emergency department presentations. Australian Health Review 31(1): 83-90.
Objective: To forecast the number of patients who will present each month at the emergency department of a hospital in regional Victoria. Methods: The data on which the forecasts are based are the number of presentations in the emergency department for each month from 2000 to 2005. The statistical forecasting methods used are exponential smoothing and Box-Jenkins methods as implemented in the software package SPSS version 14.0 (SPSS Inc, Chicago, Ill, USA).
Results: For the particular time series, of the available models, a simple seasonal exponential smoothing model provides optimal forecasting performance. Forecasts for the first five months in 2006 compare well with the observed attendance data.
Conclusions: Time series analysis is shown to provide a useful, readily available tool for predicting emergency department demand. The approach and lessons from this experience may assist other hospitals and emergency departments to conduct their own analysis to aid planning.
Aust Health Rev 2007: 31(1): 83-90.
Faddy, M. J. and S. I. McClean (2007). Using a multi-state model to enhance understanding of geriatric patient care. Australian Health Review 31(1): 91-97.
Objectives: To use multi-state Markov chain modelling to analyse data on geriatric patient care, and to make comparisons between male and female patients.
Methods: Estimation, from observed data, of covariate (age of patient and date of admission to hospital or community care) dependent parameters of statistical models for time in care and subsequent events.
Results: Differential effects of these covariates shown on the parameters of the models for female and male patients, where these parameters can be interpreted as affecting different features of the distributions of time in care.
Conclusions: Multi-state modelling is an appropriate means of analysing data on geriatric patient care and can reveal underlying patterns of differential effects, some of which may not be apparent.
Aust Health Rev 2007: 31(1): 91-97.
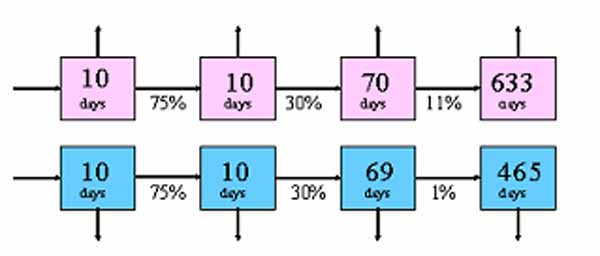
Paper: A Method for Determining an Emergency Readmission Time Window by Eren Demir, who is a PhD student with HSCMG, University of Westminster.
We are indebted to IMS MAXIMS plc's sponsorship for enabling the website version to be developed. IMS is a significant supplier to NHS and has an ongoing interest in enhancing the scope of IT support in the NHS, especially in the areas of clinical knowledge and decision support. Developers of systems looking for market opportunities are invited to contact IMS at their UK office, or by e-mail to Paul Cooper (pcooper at imsmaxims dot com). Accessing their web-site http://www.imsmaxims.com will give a feel for the scope of their work.
Some navigational notes:
A highlighted number may bring up a footnote or a reference. A highlighted word hotlinks to another document (chapter, appendix, table of contents, whatever). In general, if you click on the 'Back' button it will bring to to the point of departure in the document from which you came.Copyright (c)Roy Johnston, Ray Millard, 2005, for e-version; content is author's copyright,